
The ground-breaking research changing how we think about suicide
The ground-breaking research changing how we think about suicide
WARNING: This blog post contains themes that could be distressing for some readers. If you might be sensitive to or upset by subject matter around suicide, consider holding off on this one for now. Whether you’re the boss, a colleague, a clinician in the caring professions, an emergency service worker or simply a loved one’s family or friend, suicide is a subject that prompts universal heartache and anguish. Did you know:
- Worldwide, close to 800 000 people die due to suicide every year – that’s one person every 40 seconds.
- Last year in Australia, 65,000 people attempted suicide, and more than 3,000 died by suicide.
- Suicide is the leading cause of death for Australians (and in other developed countries) between the ages of 15 and 44.
- Young Australians are more likely to take their own life than die on our roads.
- By age 16, one in five young people have self-harmed – and by age 30, one in nine have attempted suicide.
- Depression is not the main trigger for suicide – ‘only’ 4% of people being treated for depression kill themselves. Most people who experience mental health challenges never become suicidal.
Surprised? I was. Dumbstruck.
The ripple effect
In the way that a pond is changed by a pebble, an entire community is changed by a suicide. It is estimated that on average 115-135 people are exposed to a single suicide, with one in five reporting that this experience had a devastating impact or caused a major-life disruption. Some believe this figure is a gross underestimate. Australian research found that 89% of people knew someone who had attempted suicide and 85% knew someone who had died by suicide.
Good people are dying… young and old
While we most often think of suicide as a tragedy of the young, in fact it’s their parents’ who are most at risk. The highest prevalence of suicide is in middle age. Perhaps upon nearing a half-century of life experience it’s harder to believe that despair is a passing personal crisis rather than an existential condition? For men, the peak danger period comes between the ages of 40-44 and for women it’s between 50-54. [As an aside, can anyone tell me of a campaign that is focussed on suicide prevention of women in their 50s? We’ve got the wonderful Movember, ManUp, Alright Mate, Men on the Ropes etc for our blokes. Just saying!] Young or old, male or female: every suicide deserves to be honoured with sadness and our determination to keep learning. Irrespective of age or gender there’s a complexity to suicide that is applicable across the whole lifespan. Everyone can play a part in lowering the suicide rate.
Predicting those at risk
Although suicide has been the focus of serious research for well over a hundred years and much progress has been made, we are still no better off than chance at predicting who will attempt to take their own lives. Much of the tragedy that is suicide remains unknown. Whilst in the UK last month (presenting at the 2019 British Psychological Society’s Division of Occupational Psychology Conference), I had the privilege of hearing Professor Rory O’Connell (Health Psychology, University of Glasgow) deliver the closing keynote. It was simultaneously scientifically inspiring and deeply compassionate. It had a profound effect on me, and it’s the reason for this post. As a (50-year-old!) mother-wife-daughter-sister-friend-researcher-entrepreneur-psychologist-coach and large mortgage holder, I’m desperate to share some of what I gleaned.
Suicide prevention is everyone’s responsibility
Here’s what is known:
- The risk factors leading to suicide are complex and span multiple domains – biological and biochemical (serotonin and cortisol), social and cultural (economic disadvantage and early childhood trauma), psychiatric and psychological; and they come from our past, present and future.
- Lots and lots of people think about suicide (‘ideation’) but ‘only’ about a third of those people will act on these thoughts, and in fact a landmark Australian study suggests the link is even less.
- Understanding the possible transition from thinking to doing is crucial to driving down suicide rates.
Within the context of health and wellbeing practices – or indeed any personal development or change endeavour – we are typically preoccupied with the challenge of how to get people to act on what they’re thinking without procrastinating. We want them to move as quickly as possible from having the thought to taking action. Within the context of suicide, it’s (obviously) the opposite that counts – intervening to bring about an indefinite delay to acting on thoughts. Two key questions to consider:
- What is it about the minds of the people who act on their suicidal thoughts that is different?
- How can we use these insights to achieve a reduction in suicide rates?
Inside the mind of a suicidal person
From studies of suicide notes and interviews conducted in emergency rooms with individuals in crisis who have attempted to take their life, the new research repeatedly suggests that suicide is not about wanting to die but rather about the person feeling a sense of disconnection from others, a lack of belonging and a belief they have become a burden to those around them. What Professor O’Connor explained was that there’s NEVER just one risk factor, and that the presence of risk factors only ever means a vulnerability to suicide, not an inevitability. The triggers are often small: it’s the unbearable distress arising from everyday experiences; a phenomenon referred to as the ‘kindling hypothesis’. In addition to the factors already mentioned, there are two more that demand extra attention. We’re statistically and clinically more likely to experience suicidal thoughts when we suffer from:
- ‘Socially prescribed perfectionism’: when the belief that we’re failing to meet the expectations of others is overpowering.For sufferers, it’s not what they think that’s the issue, it’s what they think we think.
In GLWS language, 9.3% of leaders in our research say they ‘Always feel driven to conform to expectations of success or perfection’ and a further 25.3% say they ‘Usually’ feel this way. More than a third of leaders may be indicating a leaning towards socially prescribed perfectionism.
- ‘Entrapment’: when we feel utterly defeated or humiliated. A sense not just of hopelessness but of being cornered, where we feel there is no escape and no alternative.A kind of tunnel vision in seeing suicide as the only option.
In GLWS language, 9.6% of leaders in our research say they
‘Never or rarely express their emotions constructively to family or friends’
Here’s the thing: entrapment is one of the very few known modifiable risk factors – supporting people to openly express their thoughts and feelings is key.
How to help keep more people safe from suicide
Despite the horrible prevalence of suicide ideation, acting on such thoughts is mercifully a much rarer event.
The crucial question becomes: ‘What influences whether or not we act on our thoughts?’
The answer is that it’s not determined by entrapment or social perfectionism. These are merely what trigger us to formulate ideas of suicide – the ‘motivational factors’ – quite different from the act of suiciding.
The transition from suicide ideation to action
In determining what factors drive the transition from ideation to action, O’Connor and his colleagues have been doing ground-breaking experimental research in the ER rooms of Scottish hospitals with people who are in crisis immediately after having attempted to, but not succeeded in, taking their life.
What they have found is that there are eight relevant ‘volitional factors’. Understanding those volitional factors will help to keep more people safe.
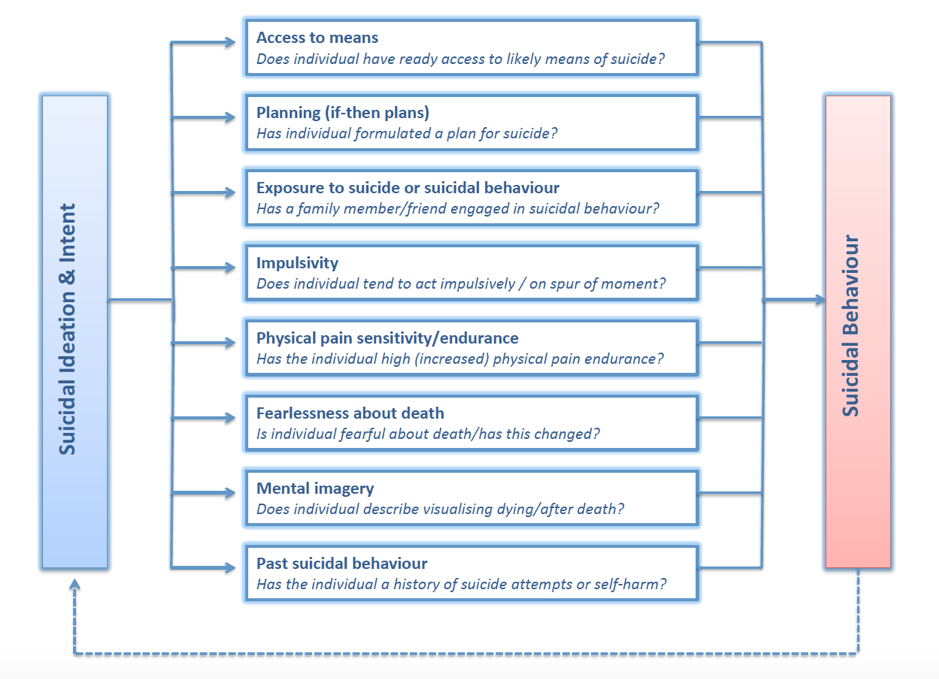
Source: The Integrated Motivational-Volitional (IMV) Model of Suicidal Behaviour O’Connor & Kirtley 2018
That old chestnut – cortisol
I briefly want to mention a fact that blew my mind:
People who are suicidal don’t release enough cortisol.
[Quick recap on the basics – when we encounter negative life events/stress, we experience a ‘Flight or Fight’ response in which our body needs to release cortisol as part of our innate coping mechanism for dealing with stress.]
People who are suicidal have a faulty cortisol system. For these people, their cortisol dysregulation means their autonomic (subconscious) nervous system releases less cortisol than control groups.
Extraordinary. It’s simply HUGE for us to know that people’s biochemical response to stress is different in people who are prone to suicidal thoughts. The interplay of physiology, biology, and psychology – the link between body and brain – never ceases to amaze. How we predict and correct for cortisol dysregulation is the next mountain to climb. There is some evidence that mindfulness helps (more on cortisol another day).
Thank you again Rory O’Connor for the important work you are doing and sharing – you are saving lives.
Everyday, practical strategies for suicide prevention
Work through the list of eight factors in the table above. Some of them you/we can do NOTHING to change: we can only understand, acknowledge and seek to accept.
For other factors, these new scientific breakthroughs can be applied immediately, using evidence-backed tips and strategies. Even small actions can alleviate some of the risk factors and here are some recommendations:
- Create a safe space at work and at home where you make a point of asking (and really listening) to others.
- Encourage people to talk and help them develop the skills and courage to express what’s going on for them and how they truly feel.
- If you have concerns, ask directly about these and the extent to which they have formulated any plans. For example:
- ‘Are you having thoughts about suicide?’ – don’t worry, you will not plant a seed or increase their risk.
- ‘Have you made a plan?’ – needs to be your second question if the answer to the first is yes.
- If you feel out of your depth, it’s okay to say so. You can acknowledge how you feel and suggest you get someone else involved who the person trusts.
- Offer to go with them or even drive them to someone for help, ideally a health professional – don’t leave them alone.
- Where impulsivity may be an issue, encourage the person to seek professional help to improve their emotional regulation. Bear in mind that three quarters of all ‘successful’ suicides are amongst men, and impulsivity is higher in adolescence males. There are forms of individual and group-based therapy with established effectiveness. Neuropsychologists are making inroads with real-time neurofeedback and brain imaging techniques.
If you are concerned about immediate danger, call the person’s doctor, a mental health service or crisis line, or dial emergency services. In Australia, BeyondBlue support a Suicide Call Back Service (1300 659 467), and Lifeline (13 11 14) and 000 are key numbers.
For more detailed help:
Heads Up have a great website with extensive resources for employers, managers, small business owners and employees available for download here https://www.headsup.org.au/supporting-others/suicide-prevention
Writing on such a complex and devastating subject that affects so many lives was a challenge that we do not take lightly, nor do we fail to appreciate the significance of bringing such a sensitive topic to you. Fundamentally, we wrote this piece to bring awareness to suicide in the hopes of getting more important suicide prevention skills and strategies into place where they’re needed the most.
We hope that by talking about this, we are playing our own part in preventing suicide – helping others to better understand suicidal behaviour, identify at-risk individuals and intervene before thought becomes action.
References:
O’Connor, R. and Portzky, G. (2018) Looking to the future: a synthesis of new developments and challenges in suicide research and prevention. Frontiers in Psychology, 9, 2139. (doi:10.3389/fpsyg.2018.02139)
https://www.australiandoctor.com.au/news/landmark-study-shakes-long-held-view-risks-suicide-ideation
Cerel, J., Maple, M., de Venne, J. van, Moore, M., Flaherty, C., & Brown, M. (2016). Exposure to Suicide in the Community: Prevalence and Correlates in One U.S. State. Public Health Reports, 131(1), 100–107. https://doi.org/10.1177/003335491613100116
Pitman A, Osborn DPJ, Rantell K, King MB. Bereavement by suicide as a risk factor for suicide attempt: a cross-sectional national UK-wide study of 3432 young bereaved adults. BMJ Open. 2016.
O’Connor, R. , Whyte, M.-C., Fraser, L., Masterton, G., Miles, J. and MacHale, S. (2007) Predicting short-term outcome in well-being following suicidal behaviour: The conjoint effects of social perfectionism and positive future thinking. Behaviour Research and Therapy, 45(7), pp. 1543-1555. (doi:10.1016/j.brat.2006.11.006) (PMID:17208199)
O’Connor, R. C. and O’Connor, D. B. (2003) Predicting hopelessness and psychological distress: The role of perfectionism and coping. Journal of Counseling Psychology, 50(3), pp. 362-372. (doi:10.1037/0022-0167.50.3.362)
https://www.theguardian.com/commentisfree/2017/sep/13/suicide-middle-aged-young-people-death
Smallwood, J., Obsonsawin, M., Baracaia, S. F., Reid, H., O’Connor, R. and Heim, D. (2003) The relationship between rumination, dysphoria, and self-referent thinking: some preliminary findings. Imagination, Cognition and Personality, 22(4), pp. 317-342. (doi:10.2190/2N80-AVM3-4A23-LEAJ)
See the GLWS™ in action now with a suite of sample reports
If you are a leader, or a coach working with leaders, you can find out how the GLWS works in practice by reviewing our suite of reports. Sign up here to get instant access.